



Peter Tari
Owner & Head Vet
Tari Vets
"I have been using Ultrasound services from VAIS for a while and quite happy. I would recommend Stefano for Ultrasound"

Lesley Burgoyne
Veterinary Surgeon
Paws Indoors
"I thoroughly enjoyed and valued the excellent teaching from Stefano at our CPD. I feel so much more confident now using the machine"

Anish Patel
Founder & Director
Max & Min Vets
"I've had the pleasure of working with Stefano at VAIS on a couple of complicated medical cases recently. He takes such care with each patient, explains findings clearly and always makes time to answer questions either myself or my team have. I would highly recommend him"
Why Choose


Diagnoses and monitors disease, localises abnormalities and guides biopsies/fluid sampling -supporting surgical planning and enabling precise, confident treatment decisions.

Evaluates intrathoracic disease - pleural effusion, pneumothorax, lung consolidation, pleural masses and pulmonary oedema - delivering detailed, timely findings to support accurate diagnosis and care.

Evaluates larynx, thyroid/parathyroid, salivary glands and cervical nodes to detect masses/cysts
(incl. parathyroid nodules), diagnose endocrine disease (e.g., hyperparathyroidism), assess laryngeal paralysis and guide minimally invasive treatments (e.g., ethanol ablation).
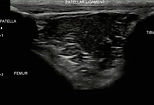
Assesses tendons, joints and soft tissues - detecting tears, inflammation and calcifications and guides sampling of deep lesions (abscesses, lymph nodes, soft-tissue/skeletal masses).




Vets: What You Get
-
On-site scan with a state of the art portable ultrasound system
-
All probes & consumables provided (no equipment needed).
-
Pre-visit details: patient prep/handling notes are sent on booking
-
Same-day PDF report
-
Images/clips for upload to your PMS
-
Vet-to-Vet case discussion
-
Post scan call with client (if required)
In-Clinic CPD: Clinical Staff
On-site CPD (3–4 hours, tailored to group size).
Practical abdominal ultrasound for small animal teams: GI & pancreas; urinary tract, adrenals & reproductive; liver, spleen; lymph nodes & vessels.
Hands-on probe time with case-based tips; printed handouts provided - lunch included. Your team leaves with clear scanning landmarks, acquisition checklists and reporting shortcuts.


Case Studies
CASE STUDY 1
Patient: 14yo (MN) DSH
Referred: Due to lethargy & hyporexia
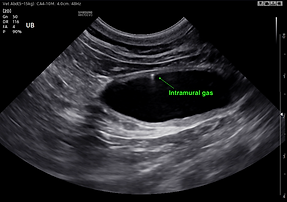
Diagnosis: Emphysematous cystitis
Additional findings: Extramural vesicourachal diverticulum
While often just an incidental finding, in this case the diverticulum it might have played a role in the development of emphysematous cystitis, along with some bladder wall mineralisation.
A rare and super interesting case. Urine culture and sensitivity showed E.Coli growth which was treated with antibiotic and anti-inflammatory. The patient made full recovery.
CASE STUDY 2
Patient: 11yo Cavachon
Referred: To investigate further PU/PD
Diagnosis: Right adrenal mass after FNAs
Fine needle aspiration was performed, as surgical excision was not an option for the owner. Cytology revealed areas suggestive of an epithelial tumour (favouring well-differentiated carcinoma), with other regions more suspicious of neuroendocrine tumour (pheochromocytoma).
This may represent a collision tumour, a rare occurrence where two distinct, non-mixed tumours exist within the same adrenal gland.
CASE STUDY 3

Patient: 5yo DSH
Referred: For vomiting and hyporexia
Diagnosis: Confirmation of no obstructive foreign body in distal jejunum and ileum
Foreign bodies typically cause obstructions and therefore dilatation of the proximal intestinal loop. When a dilated loop is encountered plus a foreign body there is no doubt that the patient needs surgery.
Things may get more complicated when the foreign body is sub-obstructive without causing dilatation of the proximal loop as the surgical call is not as clear. We identified the sub-obstruction and sign of local inflammation such as steatitis, free fluid and no intestinal peristalsis in the affected tract. We made the call for surgical intervention and the patient fully recovered.

